This is a student webpage made for an assignment at Davidson College in Dr. Campbell's Immunology Course
![]()
Overview of the Virus Ebola
Ebola belongs to a family of viruses entitled Filoviridae, and is commonly classified as a viral hemorrhagic fever (CDC, 2002). The known causes of viral hemorrhagic fever include arenaviruses, filoviruses, bunyaviruses, and flaviviruses. All virions classified as hemorrhagic are enveloped (covered) RNA viruses, whose survival is dependent on an animal reservoir. Viral hemorrhagic fever commonly describes a medical scenario in which multiple organ systems of the body are affected as well as extensive internal hemorrhaging (bleeding) (WHO,2000).
Ebola along with the Marburg virus are the only
viruses identified in the Filoviridae family (CDC,2002). Filovirus virions are
characterized by having one molecule of single stranded, negative-sense RNA,
as well as their unique "U" shaped structures (CDC, 2002).

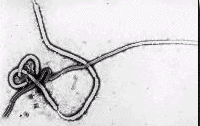
Figures 1 and 2 show scanning electron micrographs of Ebola. Figure 1 was the first photograph ever taken of Ebola in 1976.
There are four known constituents of Ebola namely: Ebola-Zaire, Ebola-Sudan, and Ebola-Ivory Coast. The fourth, Ebola-Reston (CDC,2002). Only three of the four forms listed above are known to cause disease in humans. Ebola Reston is characterized as a non-human primate infections disease. Ebola itself has an average length 920 nm and a diameter of 80 nm (WHO,2000). The virus is considered a level 4 biohazard and is only handled in the most sterile environments in full protective suiting. Ebola is spread through direct contact with blood or other bodily secretion of infected people (CDC, 2002) (WHO, 2000). This close proximity infection, makes outbreaks among small communities and families very common. Infection can also be caused through contact with contaminated medical equipment such as needles, glassware, no sterile equipment, or careless lab procedures.

Figure 3 shows scientists working with Ebola in protective clothing
Symptoms characterizing Ebola are unspecific in the first few days of the infection, making the virus even more dangerous. Infection is marked by initial signs of fever, fatigue, exhaustion, muscle aches, and dizziness (WHO,2000). As the disease progress bleeding under the skin, in internal organs, and from the eyes, ears, and mouth are seen. Patients with severe progressions of the disease express symptoms of shock, delirium, coma, seizures, and nervous system malfunction (CDC, 2002). The Ebola virus is diagnosed by specific antigens detected in blood specimens, isolation of virus in cell cultures, or detection of IgM and IgG antibodies(WHO,2000) . ELISA tests are often used to diagnose the viruses. It should be noted that all tests are conducted in the most stringent laboratory conditions in order to protect scientists and other patients. There is no established treatment for Ebola. Infected patients are treated using antiviral drugs (ribavirin) as well as generally supportive therapy that replenishes intravenous fluids, maintains blood pressure, and other bodily functions (CDC, 2002). Below is a 3D image of Ribavirin, a drug commonly used in treatment of hemorrhagic fevers, that acts as an RNA mutagen on the virion particles.
Figure 4 shows the molecular structure of the drug Ribavirin and RNA mutagen,
which is often used in treatment of hemorrhagic fevers. This figure was taken from the Protein Data Base, a government site. Click here to view the Protein Data Base
Ebola and the Immune System
Interaction of Ebola with the immune system is essential to understanding the pathogenesis of the virus. One of the characteristics of infection with the Ebola virus is the destruction of the immune system. The majority of patients infected with the virus are unable to develop sufficient immune responses. This is mainly attributed to the viruses infection of the fibroblastic reticular system, which plays a role in maximizing immune responses (Takada, 2001). Scientists speculate that disruption of cytokine production is affected by infection of both fibroblastic reticular system and mononuclear phagocytes, in addition to disruption of antigen trafficking (Takada, 2001). It is also thought that transmission of virions between tissues is partially due to infection from macrophages and circulating monocytes.
One of the primary failures of the immune system in regards the Ebola virus, is the inability to activate T-cells early in the course of the infection resulting in an insufficient humoral response which include both antibody and cytokine responses(Takada, 2001). Another result of the failure to activated T-cells adaquately is apoptosis of blood leukocytes (Takada, 2001). These characteristics of Ebola infection are commonly associated with fatality in patients. In both fatally infected patients and experimentally infected monkeys, the virus was found to cause extensive damage to lymph nodes, spleen, and bone marrow. Patients surviving infection by Ebola virions were found to develop stronger antibody responses in the early stages of infection than patients who eventually succumbed to the disease (Takada, 2001). The role of the innate immune response in the first few days of infection is considered very important in control of viral replication. Conversely up regulation of interluken 2, 10, tumor necrosis factor, and interferons are associated with infection of the Ebola virus (Takada, 2001) . Although their role is poorly understood, antibodies are thought to play an essential role in inhibiting infection of Ebola (Maruyama, 1999). Antibodies have been found that bind to the nucleoprotein, the envelope protein, and the secreted envelope glycoprotein (see Fig. 4 below). Studies have shown that neutralizing antibodies made in response to these glycoproteins are effective against the Ebola virus and show some promise in designing a vaccine (Maruyama, 1999).
Figure 56 shows a protein map of Ebola viurs RNA. (Takata, 2001) permission pending. www.bmn.com
VP35 (see diagram above) is thought to play a
pivotal role in the synthesis of viral RNA, serving as an interferon antagonist.
The production of INF antagonist is thought to be an essential factor to increasing
the pathogenicity of the Ebola Virus. There is a very strong possibility that
the potency of VP35 could account for the varying degrees of virulence among
different strains of the Ebola virus(Takada, 2001). Immunsupression of the Ebola
virus is largely attributed to a section of the glycoprotein (see diagram above:
G1 and G2), which shares a strking homology to another immunosuppressive protein
found in oncogenic retroviruses(Takada, 2001). This particular sequence is thought
to aid the Ebola virus in evading the human immune responses in addition to
suppressing the major histocompatibility complex (MHC) (Takada, 2001).
Possibilities for a Cure
Recently a protein known as cyanovirin-N found in blue-green algae has become associated with both HIV and the Ebola Virus. Cyanovirin has been found to partially inhibit the ability of both Ebola and HIV to bind and infect cells, there-by extending the host's survival time (Barrientos, 2003). Cyanovirin has been found to bind to the outside of cells there by inhibiting their ability to cross the cellular membranes (Barrientos, 2003). Cyanovirin shows promise in its ability to attatch to sugar molecules found on the surface of both HIV and the Ebola virus (Barrientos, 2003). Research trials have been preformed using animal models, in which test animals were infect with Ebola and given injections of cyanovirin once a day. This trial resulted in a delay in the onset of the disease, and longer survival in those animals injected with the protein than in those that were not injected (Barrientos, 2003) . Below is a 3D chime image of the protein Cyanovirin.
Figure 6 shows the protein Cyanovirin, which plays a potentially important role in inhibiting infection of the Ebola virus. This figure was taken from the Protein Data Base, a government site. Click here to view the Protein Data Base
Clicke here to go to the Center for Disease Control and learn more about the Ebola Virus and other hemorrhagic fevers
Refrences
Center for Disease Control. (2002) Ebola Hemorrhagic Fever. http://www.mindspring.com/~cinque/ebola.html
World Health Organization. (2000). Ebola Hemorrhagic Fever. http://www.who.int/inf-fs/en/fact103.html
Ayato Takada, A., Kawaoka, Y.B., (2001) The Pathogenesis of Ebola Hemorrhagic
Fever.
Trends in Microbiology 2001, 9:506-511 http://reviews.bmn.com/journals/atoz/browse?uid=TIM.etd00927_0966842x_v0009i10_00002201&node=TOC%40%40TIM%40011%4004%40011_04#sec_8
Maruyama T, Rodriguez LL, Jahrling PB, Sanchez A, Khan AS, Nichol ST, Peters CJ, Parren PW, Burton DR. Ebola virus can be effectively neutralized by antibody produced in natural human infection. (1999). J Virol 1999 Jul 73:6024-30 http://research.bmn.com/medline/jbrowse/record?uid=MDLN.99292898&rendertype=full
Barrientos LG, O'Keefe BR, Bray M, Sanchez A, Gronenborn AM, Boyd MR. (2003) Cyanovirin-N binds to the viral surface glycoprotein GP1,2 and inhibits infectivity of Ebola virus. Antiviral Research 2003.
