This web page was produced as an assignment for an undergraduate course at Davidson College.
Anaphylaxis
Introduction
The Canadian Pediatric Surveillance Program defines anaphylaxis as “severe systemic allergic reaction to any stimulus, having sudden onset and generally lasting less than 24 hours, involving one or more body systems and producing one or more symptoms such as hives, flushing, itching, angioedema, stridor, wheezing, shortness of breath, vomiting, diarrhea, or shock." Anaphylaxis involves multiple organ systems and is usually caused by specific antigens in sensitized individuals. Most anaphylactic reactions follow a uni-phasic reaction course. However, approximately 20% follow a biphasic course after an asymptomatic period of 1-8 hours. Protracted anaphylaxis may continue longer than 24 hours. Since anaphylaxis is a generalized reaction, anaphylaxis presents a wide variety of clinical signs and symptoms (Ellis et al., 2003). Anaphylaxis involves one or both of the following features: hypotension (which can present as fainting, collapse, or loss of consciousness) and respiratory difficulty (which may be due to laryngeal edema or asthma) (Ewan, 1998). Either respiratory obstruction or cardiovascular collapse, or both, are the cause of death. The more quickly anaphylactic symptoms appear, the more severe the reaction. In addition, patients often feel an “impending sense of death" (Ellis et al., 2003).
Anaphylaxis occurs when a person is reexposed to a specific antigen that cross-links antigen- specific IgE molecules, which are bound to mast cells and basophils. This leads to activation and degranulation of mast cells and basophils. Preformed mediators, such as histamine and tryptase, within the mast cell and basophil are released in degranulation. The metabolism of arachidonic acid in the cell membrane produces other mediators, such as prostaglandins and leukotrienes. These mediators act on receptors to induce mucus production, pruritus, vascular permeability, smooth-muscle constriction, and other symptoms of anaphylaxis (Rusznak, 2002). Rapid release of large quantities of mediators systemically will cause capillary leakage and mucosal edema, resulting in shock and asphyxia (Ewan, 1998).
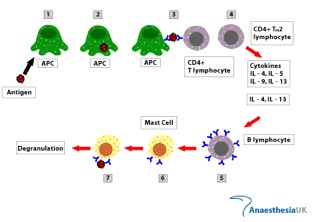
Immunological Mechanism of Anaphylaxis: (1) Antigen-presenting cell internalizes antigen. (2) The APC processes the internalized antigen. (3) The APC presents the processed peptide to CD4+ T lymphocytes via MHC II. (4) After the peptide is presented, the T cell differentiates into TH2 lymphocytes and produces IL-4, IL-5, IL-9, and IL-13. (5) IL-4 and IL-13 cause B cell immunoglobulin isotype switching to IgE. (6) The circulating IgE binds to the IgE receptors on mast cells. (7) Antigen similar to the original antigen cross-links the mast cell surface-bound IgE, resulting in cellular degranulation. Degranulation releases histamine, tryptase, and other mediators that produce the symptoms of anaphylaxis (Anaesthesia UK, 2005).
Figure 1: Overview of Immunological Mechanism of Anaphylaxis. This figure illustrates each step of the immunological mechanism for anaphylaxis. Figure taken from Anaesthesia UK( 2004), permission pending.
Mast Cell Activation
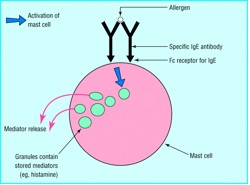
Figure 2: Activation of Mast Cell. This figure illustrates how activation of a mast cell leads to degranulation. Figure taken from Ewan(1998), permission pending.
It is important to note that anaphylactoid reactions involve activation of mast cells and release of the same mediators that cause the same effects as anaphylactic reactions, but the mechanism of mediator release in an anaphylactoid reaction is not IgE mediated. The inhibition of cyclooxygenase activity of Aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs) causes anaphylactoid reactions. Anaphylactoid reactions are also induced by radiocontrast agents, which cause direct mediator release from basophils and mast cells (Rusznak, 2002).
Etiology
The most common cause of anaphylaxis is food, which is followed by insect venom. Allergy to latex rubber is becoming a rapidly increasing problem because the use of latex rubber gloves in the medical field and also an increase in atopy. Exercise, vaccines, and semen account for rare causes of anaphylaxis. In addition, allergen immunotherapy(desensitization) may cause anaphylaxis (Ewan, 1998). See the following table outlining common causes of anaphylaxis.
Table 1 : Common Causes of Anaphylaxis. This table illustrates the common causes of anaphylaxis. Figure taken from Ewan(1998), permission pending.
Common causes of anaphylaxis
|
Foods commonly causing anaphylaxis
|
Drugs causing anaphylaxis or anaphylactoid reactions
|
Symptoms
The symptoms of anaphylaxis depend on the affected organ systems and severity of anaphylactic reaction. Monitoring patient's respiratory and cardiovascular status is critical because cardiovascular collapse or respiratory arrest could occur in severe cases. Vital signs may be normal or significantly disordered with tachypnea, tachycardia, and/or hypotension. Shock may occur without prominent skin manifestations or history of exposure. Anaphylactic patients can become restless because urticaria may cause itchiness. The release of catecholamine may cause anxiety, tremor, and a sensation of cold (Krause, 2005). The following outline explains the symptoms that may occur if a particular organ system is affected by an anaphylactic reaction.
Clinical Signs and Symptoms of Anaphylaxis According to Different Organ Systems
The Effect of Mast Cell Activation on Different Tissues
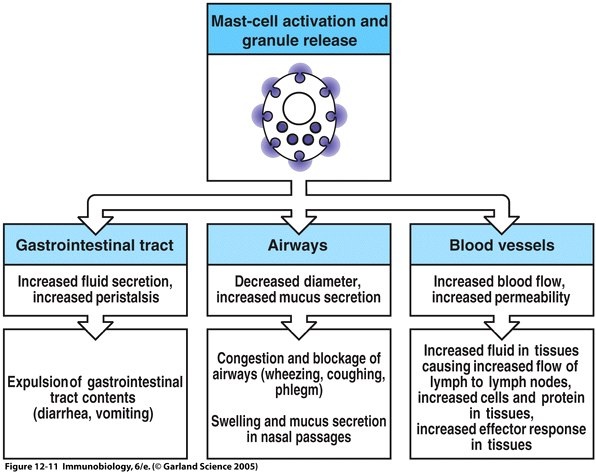
Figure 3: The Effect of Mast Cell Activation on Different Tissues. This figure illustrates how the degranulation of mast cells affects various tissues in the body. Figure taken from Janeway(2005).
The Effect of Various Molecules Released by Mast Cells During Activation
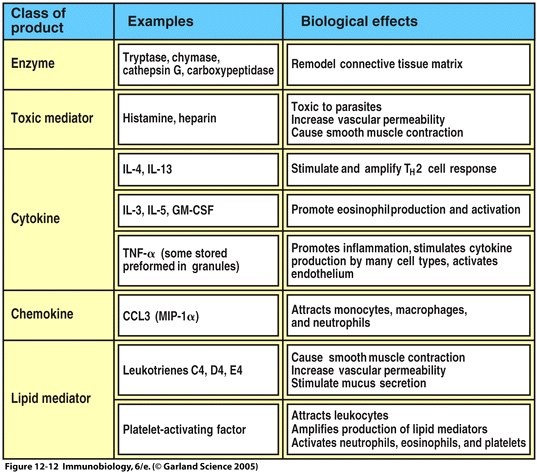
Figure 4: The Effect of Various Molecules Released by Mast Cells During Activation. This figure shows the effect of various molecules released by mast cells on activation. Figure taken from Janeway(2005).
Table 2 : Physiological Effects of Mast Cell Mediators. This table illustrates the the physiological effects, symptoms, and dangers of mast cell mediators released in an anaphylactic reaction. Figure taken from Ewan(1998), permission pending.
Physiological effect |
Clinical expression |
Danger |
Capillary leakage |
Urticaria |
|
Angio-edema |
||
Laryngeal edema |
Asphyxia |
|
Hypotension |
Shock |
|
Mucosal edema |
Laryngeal edema |
Asphyxia |
Rhinitis |
||
Asthma |
Respiratory arrest |
|
Smooth muscle contraction |
Asthma |
Respiratory arrest |
Abdominal pain |
Treatments
It is vital to be prepared and respond promptly with appropriate and aggressive treatment when treating anaphylaxis(Lieberman, 2005). The most important drug in treating anaphylaxis is epinephrine, which must be administered immediately. Epinephrine reverses the effects of anaphylaxis because it makes the heart pump faster, relaxes smooth muscle, widens air passages in the lung, contracts blood vessels,stops itching and hives, and relieves gastrointestinal cramping. After administering epinephrine, aminophylline, cortisone drugs, or antihistamines can be given to prevent acute symptoms from returning. Oxygen, intravenous fluids, and cardiac monitoring will help stabilize the heart, lungs, and blood pressure. Vasopressors and endotracheal intubation are other methods of treatment for anaphylaxis. Patients with anaphylaxis should be monitored overnight for at least six hours because there is a small chance of having a second anaphylactic reaction (Stern, 1997).
 NOTE: If this picture is too small or blurry on your web browser, check the original source for a larger and more clear image.
NOTE: If this picture is too small or blurry on your web browser, check the original source for a larger and more clear image.
Figure 5: Mechanism for Relaxation of Smooth Muscles. This figure illustrates the mechanism of how epinephrine relaxes smooth muscle. Figure taken from Bunting(2000), permission pending.
Mechanism for How Epinephrine Relaxes Smooth Muscles (See Figure 5)
Epinephrine helps control relaxation and contraction of smooth muscle cells. Contraction occurs through binding of calmodulin to Calcium ions. The Calcium-Calmodulin complex then activates the myosin light chain kinase (MLCK), which in turn phosphorylates the myosin light chains to cause contraction. When epinephrine binds to an epinephrine receptor it activates adenylyl cyclase, which produces cyclic AMP(cAMP) from ATP. Then cAMP activates a protein kinase, which phosphorylates Myosin Light Chain Kinase (MLCK). Phosphorylation inactivates MLCK so it has a lower affinity for the Calcium-Calmodulin complex. This stops the downstream signal for muscle contraction, and thus, relaxes the smooth muscle tissue. Epinephrine also decreases the release and membrane permeability of histamine to reduce the effects of histamine (Bunting, 2000).
Mechanism for How Epinephrine Raises Blood Pressure
In the mechanism of raising blood pressure, epinephrine binds a beta-adrenergic receptor, which changes shape and activates a G-Protein, which activates Adenylyl Cyclase to convert ATP to cAMP. cAMP activates cAMP-dependent protein kinase (PKA). In cardiac muscle, PKA phosphorylates calcium channels in the plasma membrane and myosin heads. Phosphorylated calcium channels remain open longer and allow more calcium into the myocyte, which uncovers more myosin-binding sites on actin. This results in more cross-bridges formed, which creates a stronger force in myocyte contraction and a high blood pressure (Davidson College Biology Department, 2006).
Prevention
In order to prevent anaphylaxis, a person should avoid substances that cause anaphylaxis and alert their doctor/ health care providers of allergies. A person may carry an anaphylaxis kit with an Epi-Pen and get allergy shots to decrease the risk of anaphylaxis and severity of reactions (Lieberman, 2005).
Works Cited
Anaesthesia UK. 2004. Management of Latex Allergy. Anaesthesia UK. Accessed 24 April 2006 <http://www.anaesthesiauk.com/article.aspx?articleid=100086%00>
Bunting, Heather et al. 2000. Epinephrine. Performance Enhancing Natural Products and Athletes. Accessed 24 April 2006 < http://www.udel.edu/chem/C465/senior/fall00/Performance1/indexa.htm.htm>
Davidson College Biology Department. Epinephrine. Bio 111 Study Guide for Spring 2006 at Davidson College. Accessed 24 April 2006 < http://bio.davidson.edu/courses/bio111/stdygd/Chapters/SG06Sp.pdf>
Ellis, Anne and James Day. "Diagnosis and Management of Anaphylaxis " Canadian Medical Association Journal 169(2003): 1-4.
Ewan,Pamela. "ABC of Allergies:Anaphylaxis" British Medical Journal 316 (1998): 1442-1445.
Janeway, C.A., Travers, P., Walport, M., Schlomchik, M. Immunobiology 6th Ed: The Immune System in Health and Disease. New York: Garland Publishing, 2005.
Krause, Richard. 29 April 2005. Anaphylaxis. eMedicine. Accessed 24 April 2006 <www.emedicine.com/emerg/topic25.htm>
Lieberman P et al. "The Diagnosis and Management of Anaphylaxis:An Updated Practice Parameter." The Journal of Allergy and Clinical Immunology 115 (2005)483-523.
Rusznak, Csaba. "Anaphylaxis and Anaphylactoid Reactions: A Guide to Prevention, Recognition, and Emergent Treatment." Postgraduate Medicine 111 (2002): 1-4.
Sampson, Hugh. "Anaphylaxis and Emergency Treatment." Pediatrics 111 (2003): 1601-1608.
Stern, David. 6 November 1997. Anaphylaxis:Life-Threatening Allergy. Asthma and Allergy Information and Research. Accessed 24 April 2006 < http://www.users.globalnet.co.uk/~aair/index.htm
If you have any questions or concerns about this web page please contact Ryan.
Return to Davidson College Biology Home Page.
Return to Immunology Home Page.
Return to Ryan's Immunology Home Page.