*this website was created as an undergraduate project for Bio307:Immunology at Davidson College*
By Amy Reid
Allergic Conjunctivitis
Introduction
Conjunctivitis, also known as pink eye, is a broad term that describes ocular disorders characterized by conjunctival inflammation. The eye is particularly vulnerable to allergic reactions because the conjunctiva are so sensitive and the eye is directly exposed to the environment. While conjunctivitis may be allergic, or non allergic, this site will focus on the causes, symptoms, immune response and treatment of allergic conjunctivitis. (American Academy of Allergy, Asthma & Immunology Inc., 2000)
In the normal eye: defense mechanisms and the conjunctiva
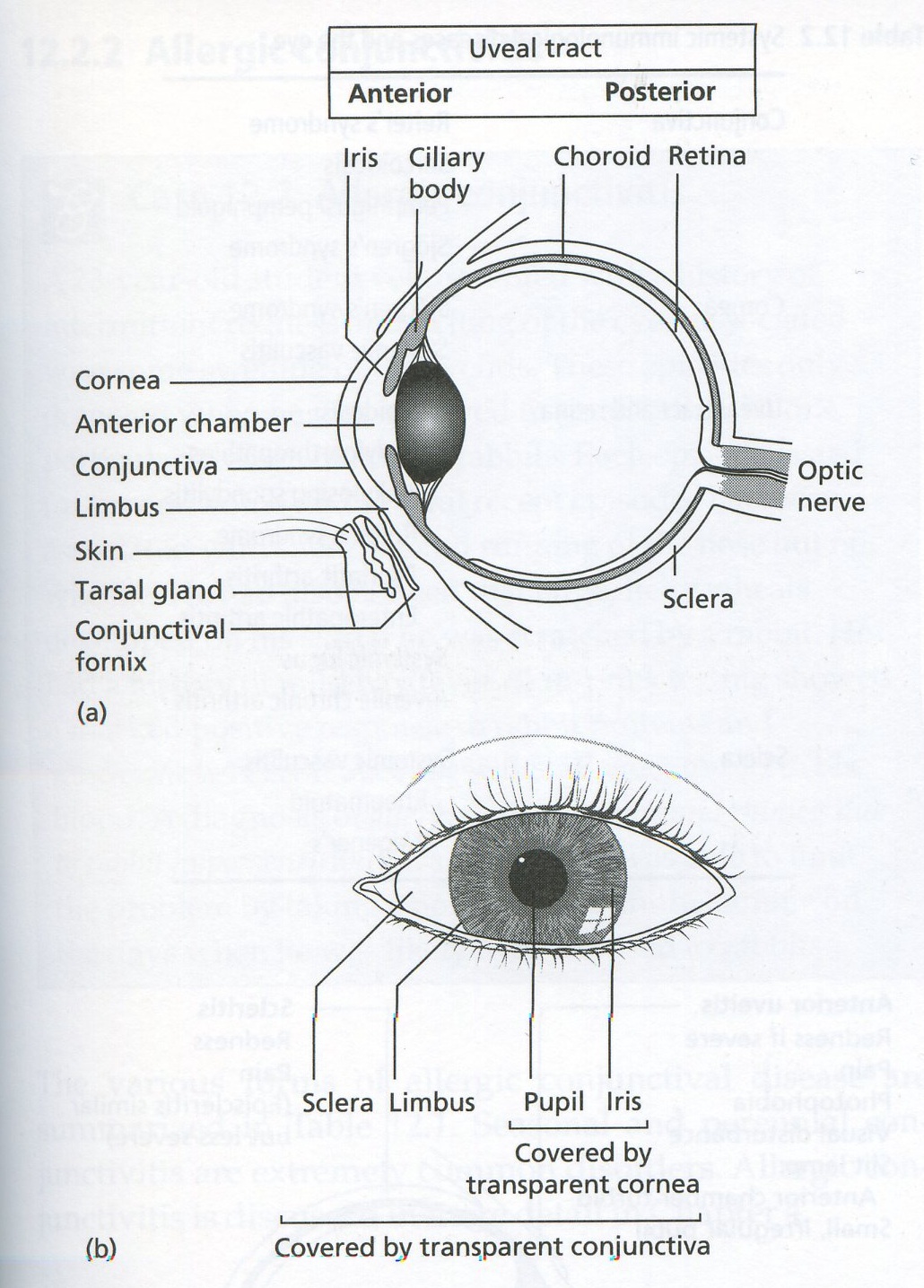
Normally, the eye is able to defend itself against infections and allergens through natural defense mechanisms. Tears contain lysozymes that prevent infection. Furthermore, they act as a lubricant that physically rids the eye of possibly harmful organisms. The eyelids and eyelashes also act as a physical barrier that protect the surface of the eye in their presence and by blinking (Friedlaender, 1995). Keeping harmful agents out, or quickly ejecting them is an important function for the protection of the eye, because an inflammatory response could disrupt retinal processes and sight. If an infection does establish itself on the eye, the extensive vascularization in the conjunctiva can quickly initiate a primary immune response initiating inflammation (Chapel et al, 1999). The conjunctiva is thin, translucent layer of tissue that lines the outer portion of the globe and the side of the eyelids that come in contact with the globe (Morrow and Abbott, 1998).
Figure 1. The anatomy of the eye. (Chapel et al, 1999)
Causes of Allergic Conjunctivitis: Airborn microorganisms & other
Allergens are antigens that are harmless, yet the immune system of some people reacts to them (Janeway et al 2005).
The allergens that initiate the immune response in allergic conjunctivitis can be present in the air or in supplies one comes into contact with everday. Airborn allergens include ragweed, pollens, pet dander, dust, and mold spores (Quinn et al, 2002). One may also develop an allergy to contacts, contact solutions, and makeup products and allergens found in one's specific work environment (AAAAI, 2000). These allergens are not 'causes' of allergic conjunctivitis in that they actively infect the eye as pathogens do, rather, certain people exhibit hypersensitivity reactions to particular allergens while others do not.
Symptoms of Allergic Conjunctivitis
General:
Allergic conjunctivitis is characterized by itchy eyes which is not a sign usually seen when the cause of conjunctivitis is bacterial or viral. Further, waking up in the morning with crusty eyes is not a sign of allergic conjunctivitis, rather of bacterial conjunctivitis. (Friedlaender, 1995). Typical of allergic conjunctivitis, patients normally have red, mildly swollen tearing eyes (Morrow and Abbott, 1998), a stringy/ropy discharge and a personal or family histry of other allergic disease (Friedlaender, 1995).
Specific:
There are five subtypes of allergic conjunctivitis.
Seasonal conjunctivitis is the most common form of allergic conjunctivitis and it is found in adults and children (Chapel et al 1999). The sympotoms are recurrent due to seasonal exposure and can can include stinging senstations and a pink or milky conjunctiva (AAAAI, 2000).
Perennial allergic conjunctivitis refers to an allergic reaction of the conjunctiva to allergens that are present all year. This form is not as widespread as seasonal conjunctivitis and is more mild (AAAAI, 2000).
Atopic keratoconjunctivitis is associated with dermatitis of the face and eyelid and usually appears in late adolescence in patients with a history of atopy (Quinn et al, 2000). A symptom of this subtype is stringy mucus discharge.
Giant papillary conjunctivitis can be a result of contact lens use, most often observed in patients wearing soft contact lenses (Quinn et al, 2000). This form of allergic conjunctivitis is thought to be an immune response to proteins that are on the inner surface of contact lenses and other ocular devices (AAAAI, 2000). One may experience slight vision blurring and abnormal conjunctiva thickening.
Vernal conjunctivitis is usually found in younger people and lasts about three to five years (Chapel et al, 1999). Most affected are males who are no longer affected by age thirty (Quinn et al, 2000). Symptoms include intense itchiness, stringy mucus discharge and "cobblestones" on the upper tarsal conjunctiva, as well as Trantas' dots, small white dots of eosinophils on the conjunctiva.
What's going on at the molecular level?
The main players: IgE, mast cells, inflammatory mediators
Antigen specific IgE medicates allergic conjunctivitis. The role of IgE was demonstrated when hypersensitivity to a particular pathogen was passively transfered to one who, previoulsy, was not allergic (Chapel et al, 1999). In addition to allergen specific IgE, some affected individuals have high levels of IgE in their tears, as is the case with vernal conjunctivitis (Chapel et al, 1999).
High levels of eosinophils in th conjunctiva tissue is a sign of allergic conjunctivitis (AAAAI, 2000). The eosinphils are effector molecules that release enzymes, cytokines and chemokines when activated to amplify the inflammatory response.
Allergic conjunctivitis is an example of soluble antigens binding to IgE and causing mast cell degranulation - Type I hypersensitivity. The allergen, pollen for example, lands on the conjunctiva. Pollen-specific IgE is attached to mast cells by FcεRI IgE receptors. When the pollen binds the IgE, the IgE cross-links and activates mast cells to release effector molecules. The released effector molecules have many functions; leukotrienes and histamine increase vascular permeability, interleukins 4 and 13 strengthen the T helper 2 cell response which then promote isotype switching to IgEs and TNF-α mediates an inflammatory response.
The redness, puffiness, and itchiness of the eyes that one experiences as symptoms of allergic conjuctivitis are all due to the inflammatory response - initiated by the activation of mast cells by the allergen. Histamine and prostaglandin production increase vascular permeability so there is more blood flow to the site - this causes redness and puffiness as more and more cells flood the area.
In addition to allergens, a genetic component may play a role in an individual's response to allergens. Families in which many generations experience allergic responses have been studied and regions of chromosomes 5 and 11, 5q and 11q, appear to have an influence on one's susceptibility to environmental allergens. Potential genes include those that encode part of the IgE receptor on chromosome 11 and one that encodes a receptor involved in smooth muscle contraction on chromosome 5. Also on chromosome 5, mutations in the promotor region of interleukin 4 have an association with higher levels of IgE.
(Janeway et al, 2005)
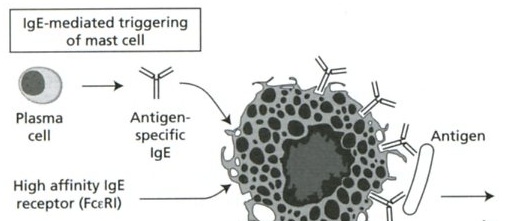
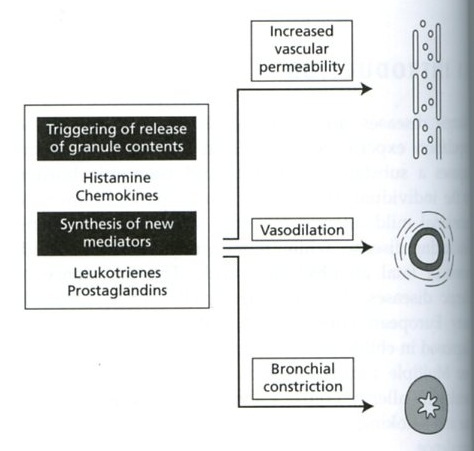
Figure 2. Schematic of mast cell activation by a soluble antigen. Plasma cells produce allergen-specific IgE. The IgE binds the receptor on the mast cell. When antigen binds the IgE and cross-links it, the degranulation of mast cells leads to vasodilation, vascular permeability and bronchial constriction. (Chapel et al, 1999)
Treatment of Allergic Conjunctivitis
Treating allergic conjuctivitis involves, at the simplest level, the avoidance of the allergen (Friedlaender, 1995). If there is more allergen, like pollen, present in the air, more IgE pollen receptors will be cross linked causing increased irritation. The goal of treatment is not to target the particular allergen to destroy it in the eye, rather to relieve symptoms; although flushing the allergen from the surface of the eye is effective to temporarily relieve symptoms (Friedlaender, 1995).
Mast Cell Stabilizers
Mast cell stabilizers like cromolyn sodium 4.0% and nedocromil 2.0% prevent the degranulation of mast cells, so fewer inflammatory mediators are released which means less puffiness, redness and itchiness. The drugs prevent the release of histamine, chemokines and platelet-activting factor (Quinn et al, 2000).
Nonsteroidal Anti Inflammatory Drugs (NSAIDs)
Prostaglandins, inflammatory mediators, are synthesized from arachidonic acid with the aid of the enzyme cyclo-oxygenase. NSAIDs are cyclo-oxygenase inhibitors. Only ketorolac has been approved by the FDA. (Quinn et al, 2000). Of 241 patients with seasonal allergic conjunctivitis surveyed, over 90% felt ketorolac as effective or more effective than other eye drops used in the past (Friedlaender, 1995).
Anti Histamines
Antihistamine medications like Levocabastine hydrochloride 0.05% decrease vascular permeability and itching caused by histamine that is released by activated mast cells. These drugs are histamine receptor agonists that block H1 histamine receptors in the conjunctiva and eyelid (Quinn et al, 2000). These can be taken orally or applied topically and provide fast itch relief (AAAAI, 2000).
Corticosteroids
Corticosteroids inhibit inflammation and decrease lymphocyte migration to the site of inflammation. They also block phospholipase A2 activity which inhibits prostaglandin synthesis by affecting the arachidonic acid path (Quinn et al, 2000). This form of treatment is only used for severe allergic conjunctivitis and not long-term becuase of the potential for cataracts, glaucoma and infections of the cornea (AAAAI, 2000).
Allergen Immunotherapy
Allergen immunotherapy is also known as desensitization therapy becuase that is the goal of the therapy. Through frequent small doses that are slowly increased in amount, the allergic reaction is reduced (Muth, 2002). This therapy is for patients when nothing else works and can provide great benefits for those suffering from seasonal and perennial allergic conjunctivitis (AAAAI, 2000).
Conclusions
Allergic conjunctivitis is caused by an allergic response to common environmental microorganisms. The allergen binds gE receptors that are bound to mast cells. These mast cells are activated and initiate an inflammatory response that leads to the symptoms associated with allergic conjunctivitis. Hypersensitivity and a specific IgE response is not a reaction that all have. This has led to genetic analyses that have revealed a potential genetic component in atopy. There is still so much that is not understood about allergic reactions - this plus the fact that over 50 million Americans suffer from allergies each year (AAAAI, 2000) will keep research in this field profitable. Although, if allergies could be cured, would that be desirable from the perspective of the drug makers?
*this website was created as an undergraduate project for Bio307:Immunology at Davidson College*
Sources
Morrow GL and Abbott RL. 1998 Feb 15. Conjunctivitis. American Family Physician 57(4). <http://www.aafp.org/afp/980215ap/morrow.html> Accessed 2006 Apr 23.
American Academy of Allergy, Asthma and Immunology (AAAAI). 2000. The Allergy Report: Volume 3 Conditions that may have an allergic Component. <http://www.aaaai.org/ar/volume3.pdf> Accessed 2006 Apr 23.
American Optometric Association. Quinn CJ, Mathews DE, Noyes RF, Oliver GE, Thimons Jr JJ, Thomas RK (The American Optometric Association Consensus Panel on Care of the Patient with Conjunctivitis). Care of the Patient with Conjunctivitis. <http://www.aoa.org/documents/CPG-11.pdf> Accessed 2006 Apr 23.
Chapel H, Haeney M, Misbah S and Snowden N. Essentials of Clinical Immunology. 4th ed. London: Blackwell Science Ltd; 1999. p. 78, 82, 222-225.
Muth, AS, Ed. 2002. Allergies sourcebook. Detroit, MI: Omnigraphics. p. 101-103.
Janeway CA, Travers P, Walport M, Shlomchik MJ. Immunobiology: The Immune System in Health and Disease. 6th ed. NewYork: Garland Science Publishing; 2005. p.517-541.
Friedlaender MH . A Review of the Causes and Treatment of Bacterial and Allergic Conjunctivitis. Clinical Therapeutics. 1995;17:5 800-10.